File: <leishmaniasis.htm> <Medical Index> <General Index> Site Description Glossary <Navigate
to Home>
|
LEISHMANIASIS & Sandflies (Contact) Please
CLICK on
underlined links for details: Cutaneous Leishmaniasis Diffuse
Cutaneous Leishmaiasiss Mucocutaneous Leishmaniasis Visceral
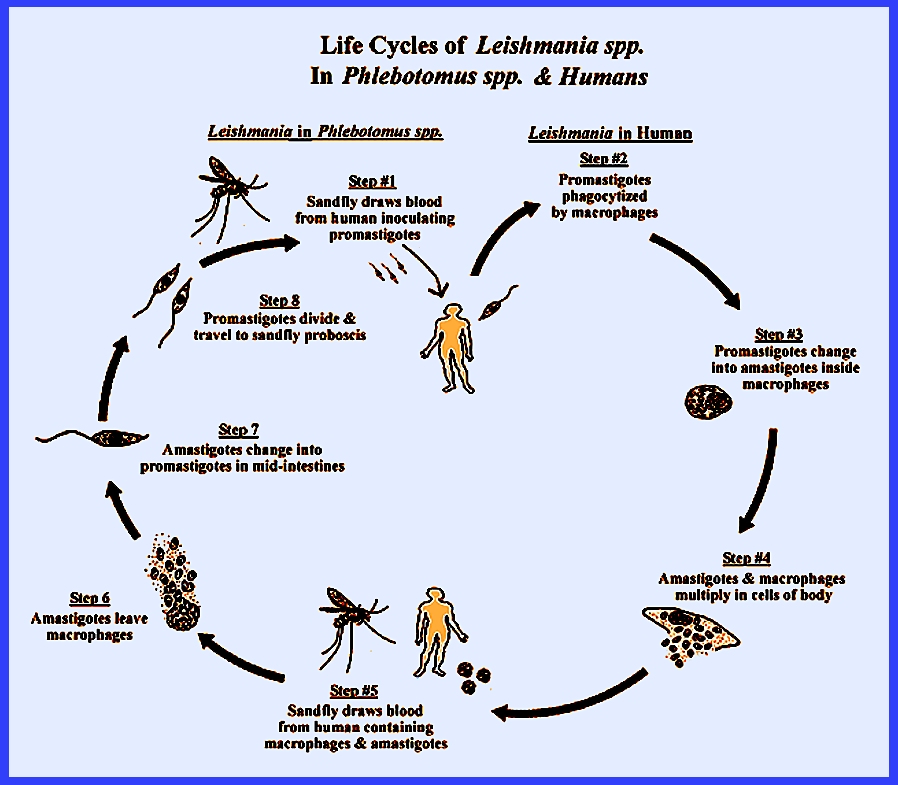
Leishmaniasis The life
cycle begins when amastigote
parasites are ingested by female sand flies during a blood meal. the parasites multiply in the sandfly
intestines and turn into promastigotes,
which are elongated and have a flagellum that attaches to the mid- or
hind-intestinal wall where they multiply.
Those that are not voided migrate to the anterior mid-intestines and
then to the fore-intestines. There
some parasites change into metacyclic
forms. After 4-12 days after
the sandfly has has an infected blood meal the metacyclic forms are found in
the mouthparts from which they may be introduced to a new host during feeding. Transmission is maximized because infected
sandflies probe more frequently.
Because sandflies also feed on plants containing sugar, this aids
parasite development. (Also see Life
Cycle) Most
leishmaniasis are zoonoses,
and the degree of human involvement varies in different areas (Service
2008). The epidemiology is mostly
determined by the sandfly species, their ecology and behavior as well as the
strains of Leishmania
parasites. Sometimes the sandflies
transmit infections mostly among wild or domestic animals with little human
involvement. In other areas the
animals may serve as reservoir hosts for human infection. The disease may also be transmitted
between people by sandflies with animals taking no part in its transmission
(e.g., India). Following are more
details concerning the different forms of the disease as given by Service
(2008): Sometimes
known as "Oriental
Sore" this form of leishmaniasis occurs principally in arid
parts of the Middle East to India, Asia and Africa. The principal parasites are Leishmania
major, which are vectored by Phlebotomus
papatasi, and Leishmania
tropica is vectored by Phlebotomus sergenti. Leishmania
major is mainly zoonotic and gerbils are the reservoir hosts. Leishmania
tropica is in densely populated areas where humans are the
principal reservoir hosts. In America
the cutaneous form occurs mainly in forested parts of Mexico south to
northern Argentina. It is caused by Leishmania braziliensis (= amazoniensis) and Leishmania mexicana. Dogs and rodents are probably the
principal reservoir hosts. The main
vectors are Lutzomyia wellcomei
and Lutzomyia flaviscutellata. This is a very
severe form of the disease that occurs from Mexico to Argentina and is caused
by Leishmania braziliensis. Dogs are reservoir hosts and Lutzomyia wellcomei a principal vector. Diffuse Cutaneous Leishmaiasiss Cutaneous nodules all over the body
characterize this form. It occurs in
Venezuela, the Dominical Republic and the highlands of Ethiopia and Kenya. In South America the parasite is Leishmania amazonensis, which is
vectored by Lutzomyia flaviscutellata. Spiny rats are reservoir hosts. In Africa the parasite is Leishmania aethiopica vectored by Phlebotomus pedifer and P. longipes. Rock hyraxes are reservoir hosts. Also known as "kala-azar"
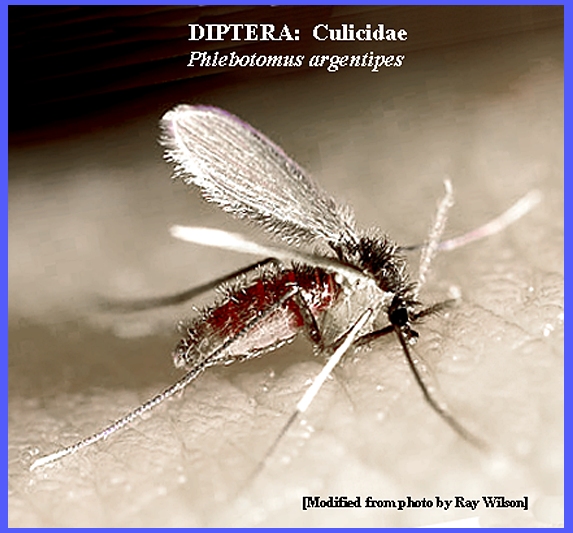
this form is caused by Leishmania donovani
donovani. It occurs in
India, Sudan, Ethiopia and East Africa.
Vector species include Phlebotomus
argentipes and Phlebotomus
orientalis. Wild cats,
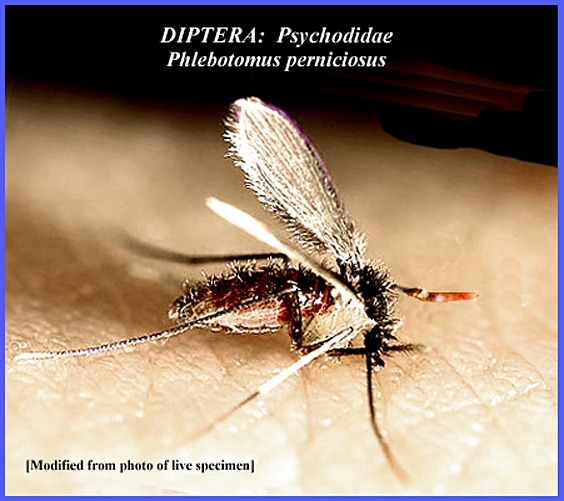
genets and rodents may be the main reservoir hosts. In the Mediterranean area and central Asia Leishmania donovani infantum is the
parasite , which is vectored by Phlebotomus
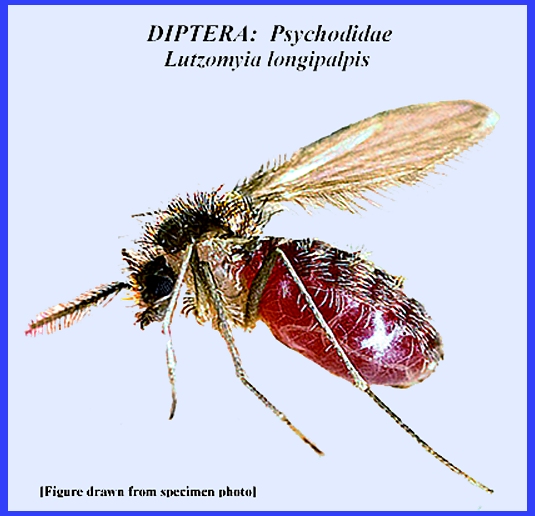
ariasi and Phlebotomus perniciosus. Foxes and dogs are reservoir hosts. This form also occurs at times in Central
and South America where the parasite is Leishmania
donovani infantum and is vectored by species of the Lutzomyia longipalpis
complex (Service 2008). Control or avoidance of the sandfly
vectors is required to reduce incidence of infection (Alexander & Maroli
2003). Insecticidal control of vector
sandflies is effective until resistance sets into the fly population. Therefore, the use of repellants is
preferable. To reduce diseases caused
by sandflies some efforts have been made to eliminate reservoir hosts from
populated areas. Further efforts to
control the vectors remain experimental, especially as the breeding sites of
most sandflies are not easily found. Lieshmania
& Phlebotomus - Life Cycles = = = = = = = = = = = =
= = = = = = = = Key References: <medvet.ref.htm> <Hexapoda> Alexander, B. & M. Maroli. 2003.
Control of phlebotomine sandflies.
Med. & Veterinary Entomology 17:
1-18. Ashford, R. W.
2001. Leishmaniasis. 2001. IN: Encycl. of
Arthropod Transmitted Infections of Man & Domesticated Animals. CABI pp. 269-79. Guerin, P.
J., P. Olliaro & S. Sundar et
al. 2002. Visceral leishmaniasis: current status of
control, diagnosis & treatment, & a proposed research & development agenda. Lancet Infect. Diseases 2: 494-501. Hide, G, J. C. Mottram, G. H.
Coombs & P. H. Holmes. 1996. Trypanosomiasis and Leishmaniasis. Biol. & Control, Wallingford: CAB internat. Killick-Kentrick, R.
1999. The biology
of phelebotomine sand flies. Clinics
in Dermatology 17: 279-89. Lainson, R. 1983. The American leishmaniases: some
observations on their ecology and epidemiology. trans. Roy Soc. Trop. Med.
Hyg. 77: 569-96. Lane, R. P.
1991. The contribution of
sand-fly control to leishmaniasis control.
Ann. Soc. Belge de Medicine Trop. 71:
65-74. Legner, E. F. 1995.
Biological control of Diptera of medical and veterinary importance. J. Vector Ecology 20(1): 59_120. Legner, E. F. 2000.
Biological control of aquatic Diptera. p. 847-870.
Contributions to a Manual of Palaearctic Diptera, Vol. 1, Science
Herald, Budapest. 978 p. Matheson, R. 1950.
Medical Entomology. Comstock
Publ. Co, Inc. 610 p. Service, M.
2008. Medical Entomology For
Students. Cambridge Univ. Press. 289 p Tayeh, A., L.
jalouk & A. M. Al-Khiami. 1997.
Cutaneous leishmaniasis control trial using pyrethroid-impregnated
bednets in villages near Aleppo, Syria. WHO/LEISH 97.41. Geneva: WHO Div. of Control of Tropical Diseases. Ward, R. D.
1990. Some aspects of the
biology of phlebotomine sand-fly vectors.
Adv. Dis. Vector Res. 6:
91-126. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}